×
Il semble que vous utilisiez une version obsolète de internet explorer. Internet explorer n'est plus supporté par Microsoft depuis fin 2015. Nous vous invitons à utiliser un navigateur plus récent tel que Firefox, Google Chrome ou Microsoft Edge.

Devenez membre d'Incathlab et bénéficiez d'un accès complet !

Vous devez être membre pour accéder aux vidéos Incathlab sans limitation. Inscrivez vous gratuitement en moins d'une minute et accédez à tous les services Incathlab ! Vous avez aussi la possibilité de vous connecter directement avec votre compte facebook ou twitter en cliquant sur login en haut à droite du site.
Inscription Connexion
Inscription Connexion
Protocol
- Procedure time: 165 min
- Exposure time: 36 min
- Exposure: 349 mGray
-
Contrast volume: 2000 ml
Date du tournage : 29/06/2018
Dernière mise à jour : 09/06/2021
Dernière mise à jour : 09/06/2021

Participer à la discussion
Suggestions

Vendredi 4 avril 2025 de 13h à 15h (GMT+2)
Honolulu : Vendredi 4 avril 2025 de 02h à 04h (GMT+2)
San Francisco : Vendredi 4 avril 2025 de 05h à 07h (GMT+2)
New York : Vendredi 4 avril 2025 de 08h à 10h (GMT+2)
Buenos Aires : Vendredi 4 avril 2025 de 09h à 11h (GMT+2)
Reykjavik : Vendredi 4 avril 2025 de 12h à 14h (GMT+2)
London / Dublin : Vendredi 4 avril 2025 de 13h à 15h (GMT+2)
Paris / Berlin : Vendredi 4 avril 2025 de 14h à 16h (GMT+2)
Istanbul : Vendredi 4 avril 2025 de 15h à 17h (GMT+2)
Moscou / Dubaï : Vendredi 4 avril 2025 de 16h à 18h (GMT+2)
Bangkok : Vendredi 4 avril 2025 de 19h à 21h (GMT+2)
Shanghai : Vendredi 4 avril 2025 de 20h à 22h (GMT+2)
Tokyo : Vendredi 4 avril 2025 de 21h à 23h (GMT+2)
Sydney : Vendredi 4 avril 2025 de 23h à 01h (GMT+2)
Wellington : Samedi 5 avril 2025 de 01h à 03h (GMT+2)
San Francisco : Vendredi 4 avril 2025 de 05h à 07h (GMT+2)
New York : Vendredi 4 avril 2025 de 08h à 10h (GMT+2)
Buenos Aires : Vendredi 4 avril 2025 de 09h à 11h (GMT+2)
Reykjavik : Vendredi 4 avril 2025 de 12h à 14h (GMT+2)
London / Dublin : Vendredi 4 avril 2025 de 13h à 15h (GMT+2)
Paris / Berlin : Vendredi 4 avril 2025 de 14h à 16h (GMT+2)
Istanbul : Vendredi 4 avril 2025 de 15h à 17h (GMT+2)
Moscou / Dubaï : Vendredi 4 avril 2025 de 16h à 18h (GMT+2)
Bangkok : Vendredi 4 avril 2025 de 19h à 21h (GMT+2)
Shanghai : Vendredi 4 avril 2025 de 20h à 22h (GMT+2)
Tokyo : Vendredi 4 avril 2025 de 21h à 23h (GMT+2)
Sydney : Vendredi 4 avril 2025 de 23h à 01h (GMT+2)
Wellington : Samedi 5 avril 2025 de 01h à 03h (GMT+2)
The Drug Eluting Technology Show
Partager
Attempted recanalization of chronically thrombosed limb of Iliocaval reconstruction
Dr Thulasidasan & Dr Karunanithy
Partager
Recanalisation and stenting of chronically-occluded right iliac veins in a patient with severe post-...
Dr Thulasidasan & Dr Karunanithy
Partager
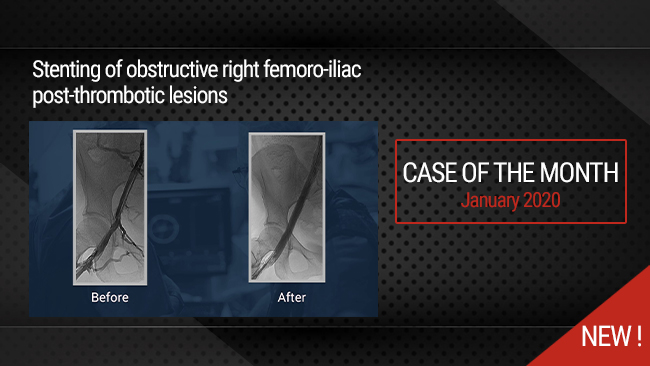
Stenting of obstructive right femoro-iliac post-thrombotic lesions
Case of the month: January 2020
Partager
Up-and-over SAFARI to recanalize and stent a long-segment BTK occlusion in a patient with CLOI
Dr Thulasidasan & Dr Karunanithy
Partager
{kind=link}
Live case #4: Calcified popliteal artery occlusion
MULTI-LEVEL CTO Endovascular course 2024
Partager
Drug-Eluting Technologies in PAD: DES and DCB vs BMS and POBA
by Dr. Athanasios Diamantopoulos
Partager
K R. Why did we deploy stent in pop ata and tpt. There is no flow limiting dissection or >30% residual lesion in pop and tibial vessels after plasty. You could have left it there. Leaving even non flow limiting dissection is acceptable in tibials. The idea behing doing BTK is just to heal the foot lesion which could be achieved with plasty alone as you did
Deploying stent actually adds time, contrast and radiation exposure , cost on procedure. Does not any therapeutic benefit. And one more thing no need for DCB plasty for tibials.
mohamad ali A. its a good point i guess he wouldnt deploy it if there wasnt a plan of kissing for ata and tpt
Venkatesa R. very good