×
Il semble que vous utilisiez une version obsolète de internet explorer. Internet explorer n'est plus supporté par Microsoft depuis fin 2015. Nous vous invitons à utiliser un navigateur plus récent tel que Firefox, Google Chrome ou Microsoft Edge.
My Player placeholder

Devenez membre d'Incathlab et bénéficiez d'un accès complet !

Vous devez être membre pour accéder aux vidéos Incathlab sans limitation. Inscrivez vous gratuitement en moins d'une minute et accédez à tous les services Incathlab ! Vous avez aussi la possibilité de vous connecter directement avec votre compte facebook ou twitter en cliquant sur login en haut à droite du site.
Inscription Connexion
Inscription Connexion
39867 vues
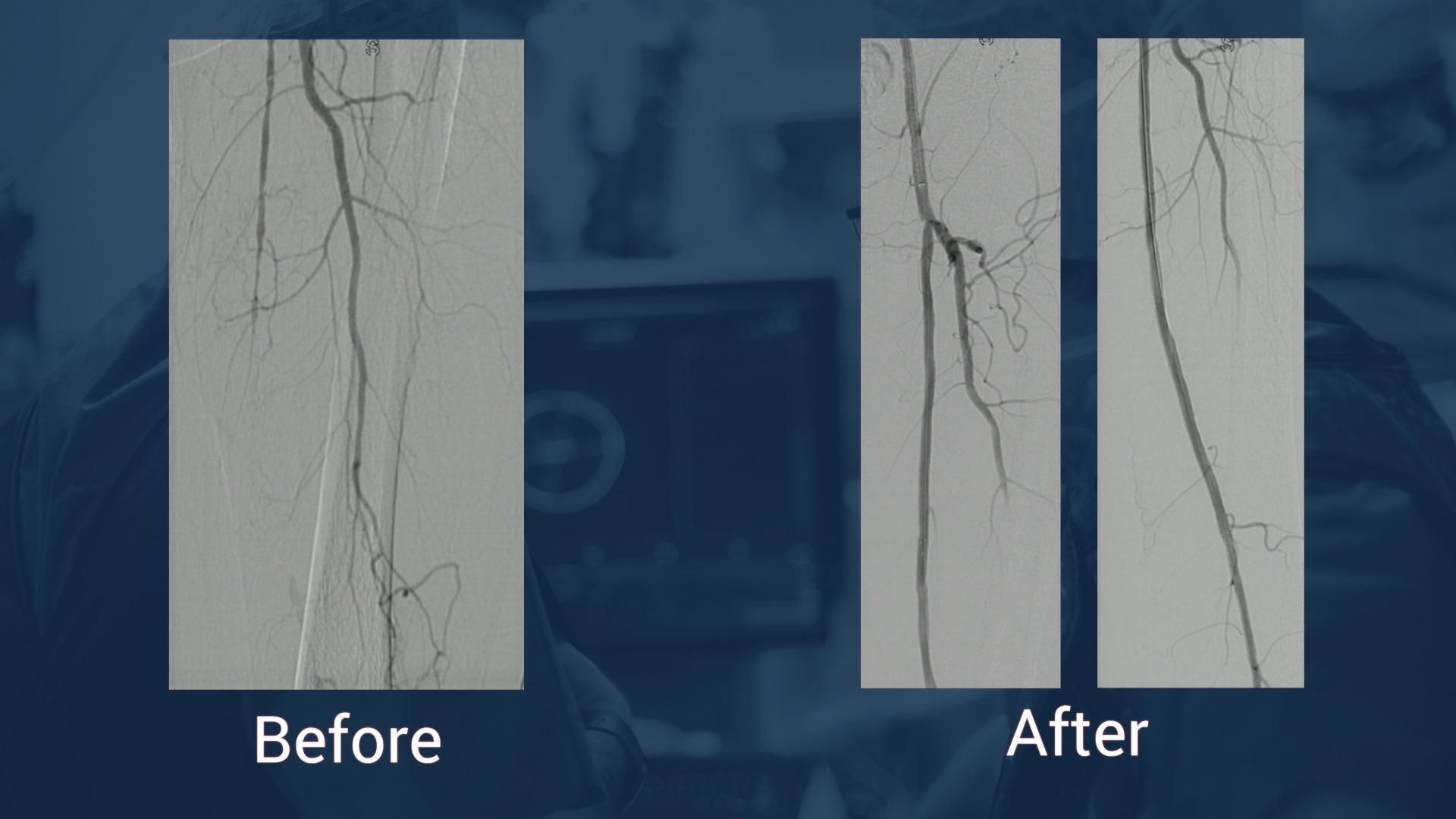
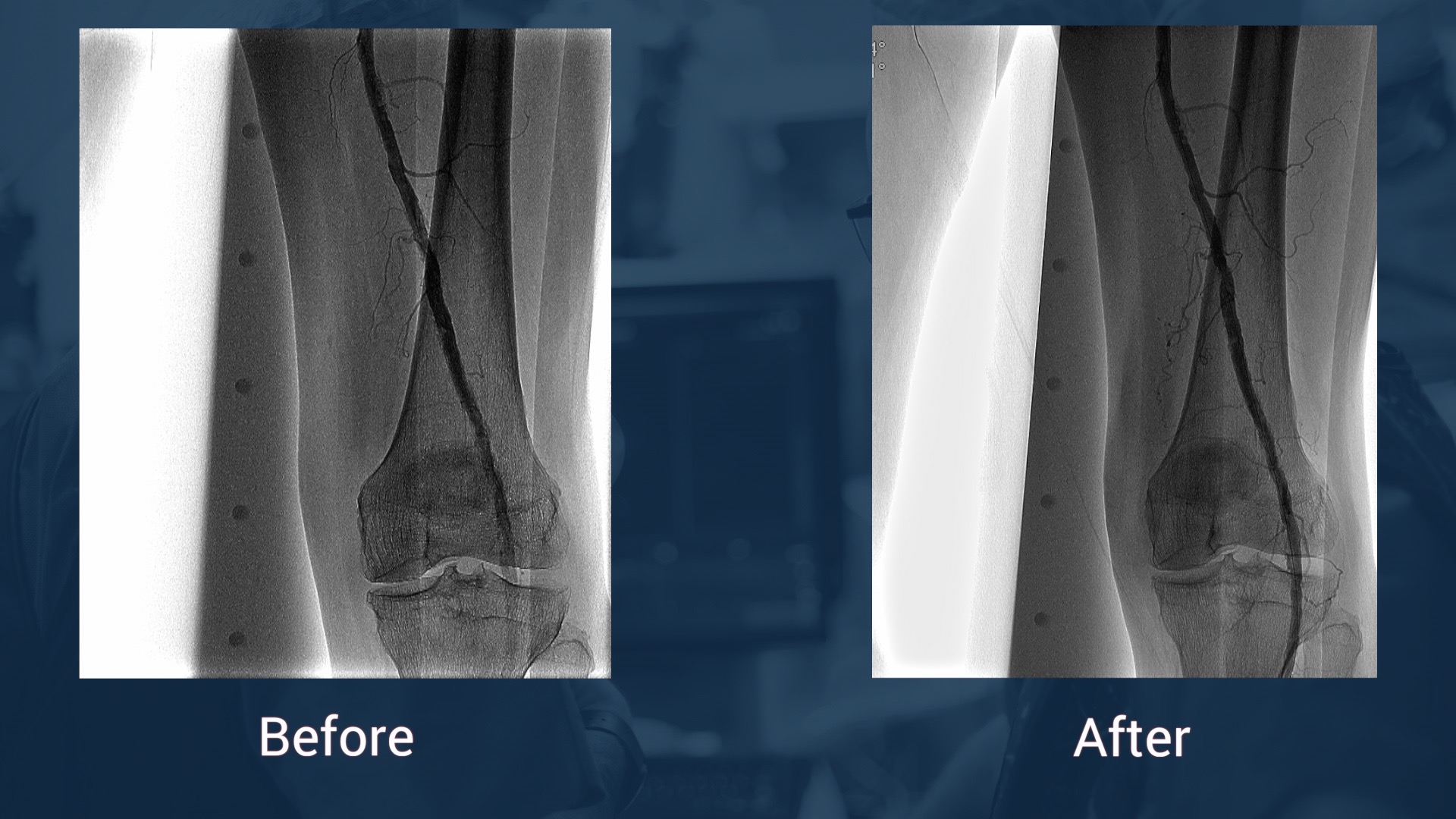
This 18 minutes didactic procedure concerns a 78 years old male with extremely severe peripheral artery disease: a Left limb amputation and a Right limb trophic ulcer. He presents Three right consecutive artery occlusions: Mid-SFA, Popliteal, proximal and distal posterior tibial.
This extremely complex case was treated using different technics according to the arterial segment: Sub intimal angioplasty and long stenting for SFA, Drug coated balloon for Popliteal, DES for proximal posterior tibial and coronary technics for plantar arteries.
Step-by-Step Procedure
- Right Antegrade femoral access
- Pre-procedure discussion of strategy for a multilevel artery occlusion
- Guide wire selection and escalation for crossing
- Support micro-catheter selection
- Pre-dilatation of more than 50cm with low profile long balloon
- Technics to re--enter in foot arteries
- DES for distal leg arteries
- DCB for popliteal artery
- Self-expandable drug eluting stent for dissection and residual stenosis of SFA
Learning points
- Selection and feasibility of antegrade femoral access
- Guide Wire and micro-catheter selection for multilevel crossing
- Balloon angioplasty with low profile long balloons
- Technics to re-enter in plantar artery
- Use of DCB (Drug Coated Balloon) for popliteal artery
- Use of balloon DES in tibial artery
- Self -expandable DES at the femoral level
Biobliography
-
Short-Term Results of Eluvia™ Paclitaxel-Eluting Stent in External Iliac and Femoropopliteal Lesions - Article
Elens M, Verhelst R, Possoz J, Mastrobuoni S, Lacroix V, Astarci P.
Surg Technol Int. 2017 Nov 9;31. pii: sti31/894. [Epub ahead of print]
-
Drug-coated balloon angioplasty for the management of recurring infrapopliteal disease in diabetic patients with critical limb ischemia - Article
Palena LM, Diaz-Sandoval LJ, Gòmez Jabalera E, Peypoch Perez O, Sultato E, Brigato C, Brocco E, Manzi M.
Cardiovasc Revasc Med. 2017 Jun 20. pii: S1553-8389(17)30196-3. doi: 10.1016/j.carrev.2017.06.006. [Epub ahead of print]
-
Innovations in the Endovascular Management of Critical Limb Ischemia: Retrograde Tibiopedal Access and Advanced Percutaneous Techniques - Article
Mustapha JA, Diaz-Sandoval LJ, Saab F.
Curr Cardiol Rep. 2017 Aug;19(8):68. doi: 10.1007/s11886-017-0879-1.
-
Innovations in the Endovascular Management of Critical Limb Ischemia: Retrograde Tibiopedal Access and Advanced Percutaneous Techniques - Article
Mustapha JA, Diaz-Sandoval LJ, Saab F.
Curr Cardiol Rep. 2017 Aug;19(8):68. doi: 10.1007/s11886-017-0879-1.
-
Angiosome-directed revascularization in patients with critical limb ischemia - Article
Jongsma H, Bekken JA, Akkersdijk GP, Hoeks SE, Verhagen HJ, Fioole B.
J Vasc Surg. 2017 Apr;65(4):1208-1219.e1. doi: 10.1016/j.jvs.2016.10.100.
Date du tournage : 05/12/2016
Dernière mise à jour : 31/01/2018
Dernière mise à jour : 31/01/2018




Our Cases of the Month
The case of the month is a new way for our users to watch, learn, and share with incathlab. They can watch a video that highlights an innovative case and uses excellent pedagogical techniques, lear...
Partager
Participer à la discussion
Suggestions
Provisional Bifurcation techniques to support bailout scenarios
Insights from the Visible Heart�...
Case of the month: July 2024
Partager
Complex Aorto-iliac lesion: How to deal with symptomatic Abdominal Aortic calcified stenosis extendi...
Case of the month: November 2018
Partager
Calcified distal Left Main and LAD stenoses - Rotablation treatment and IVUS evalutation
Case of the month: June 2017
Partager
{kind=link}
{kind=link}
{kind=link}
Alaaeldin H. what is the expected patency for this long segment ,multilevel occlusion.
Max A. Thank you for your comment. This patient requires a monthly follow up to maintain patency in order to assure ulcer healing . After 6 months the risk of restenosis and occlusion is high .
marcus P. Set good
Sandeep S. why did we have to break the end of Eluvia stent towards the end of deployment.
Georgi G. Leave a new comment to the discussion
Max A. It appears to be more convenient in long ELUVIA stent.
Collu B. Congratulations for very informative case