×
It looks like you're using an obsolete version of internet explorer. Internet explorer is no longer supported by Microsoft since the end of 2015. We invite you to use a newer browser such as Firefox, Google Chrome or Microsoft Edge.

Become an Incathlab member and receive full access to its content!

You must be an Incathlab member to access videos without any restrictions. Register for free in one minute and access all services provided by Incathlab.You will also be able to log into Incathlab from your Facebook or twitter account by clicking on login on the top-right corner of Incathlab website.
Registration Login
Registration Login
19137 views
This didactic procedure concerns a 62 years old man, presenting severe right limb intermittent claudication (Rutherford 3) & long proximal SFA lesion with subsequent short occlusion.
It was treated by contralateral and retrograde approach, the lesion was prepared with directional atherectomy & a new cutting balloon (Chocolate-Medtronic). A good final result was obtained with DCB angioplasty.
Educational objectives
- How to deal with extensive SFA disease.
- How to performSFA retrograde puncture, crossing and guidewire externalization.
- Effectivness of Directional atherectomy in long SFA lesions.
- Optimal vessel preparation with combined atherectomy & cutting balloon.
- How to leave Nothing behind.
Step-by-Step description
- Left femoral access 7F (Contralateral approach).
- Crossover approach with 6F long sheath assisted by Admiral 6x40mm balloon.
- Approach lesion with 0.018" Command guidewire supported by Trailblazer microcatheter.
- After Command & Connect guidewires failure, a retrograde approach is decided.
- Retrograde puncture of the distal right SFA.
- Retrograde crossing of the lesion & externalization of the command over a BER catheter.
- Filter placment in the distal popliteal artery.
- predilatation with 3.5mm balloon of the occluded zone.
- Directional atherectomy using a HawkOne device 7F.
- Balloon dilatation with a 5x80mm balloon : distal & proximal SFA.
- Second directional atherectomy run.
- Distal SFA dilatation with Chocolate 6x40mm balloon (Medtronic).
- Multilevel dilatation with DCB : IN PACT Pacific 5x120mm (Medtronic)
- Distal filter retreiving Spider 7mm (Medtronic).
- Final angiographic control.
Protocol
- Procedure time: 90 min
- Exposure time: 29 min
- Exposure: 321 mGy
-
Contrast volume: 120 ml
Biobliography
-
-
Combined HawkOne directional atherectomy and paclitaxel-coated balloon angioplasty for isolated calcified popliteal artery lesion: a no-stent approach to lower extremity endovascular revascularization. - Article
Authors: Loffroy R, Chevallier O, Falvo N, Gehin S, Midulla M, Galland C.
Publication:doi: 10.21037/qims.2018.03.10.
-
Directional Atherectomy Followed by a Paclitaxel-Coated Balloon to Inhibit Restenosis and Maintain Vessel Patency: Twelve-Month Results of the DEFINITIVE AR Study. - Article
Authors: Zeller T, Langhoff R, Rocha-Singh KJ
Publication doi:10.1161/CIRCINTERVENTIONS.116.004848.
-
Debulking Atherectomy in the Peripheral Arteries: Is There a Role and What is the Evidence? - Artice
Authors: Katsanos K, Spiliopoulos S, Reppas L, Karnabatidis D.
Publication doi: 10.1007/s00270-017-1649-6. Epub 2017 Apr 27.
-
Combined treatment of heavy calcified femoro-popliteal lesions using directional atherectomy and a paclitaxel coated balloon: One-year single centre clinical results. - Article
Authors: Cioppa A, Stabile E, Popusoi G, Salemme L, Cota L
Publication doi: 10.1016/j.carrev.2012.04.007. Epub 2012 May 25.
-
A prospective, multi-center study of the chocolate balloon in femoropopliteal peripheral artery disease: The Chocolate BAR registry. - Article
Authors: Mustapha JA, Lansky A, Shishehbor M, Miles McClure J, Johnson S, Davis T, Makam P, Crowder W, Konstantino E, Attaran RR; Chocolate Bar Investigators.
Publication doi: 10.1002/ccd.27565. Epub 2018 Mar 7.
Shooting date : 2018-10-09
Last update : 2021-05-11
Last update : 2021-05-11







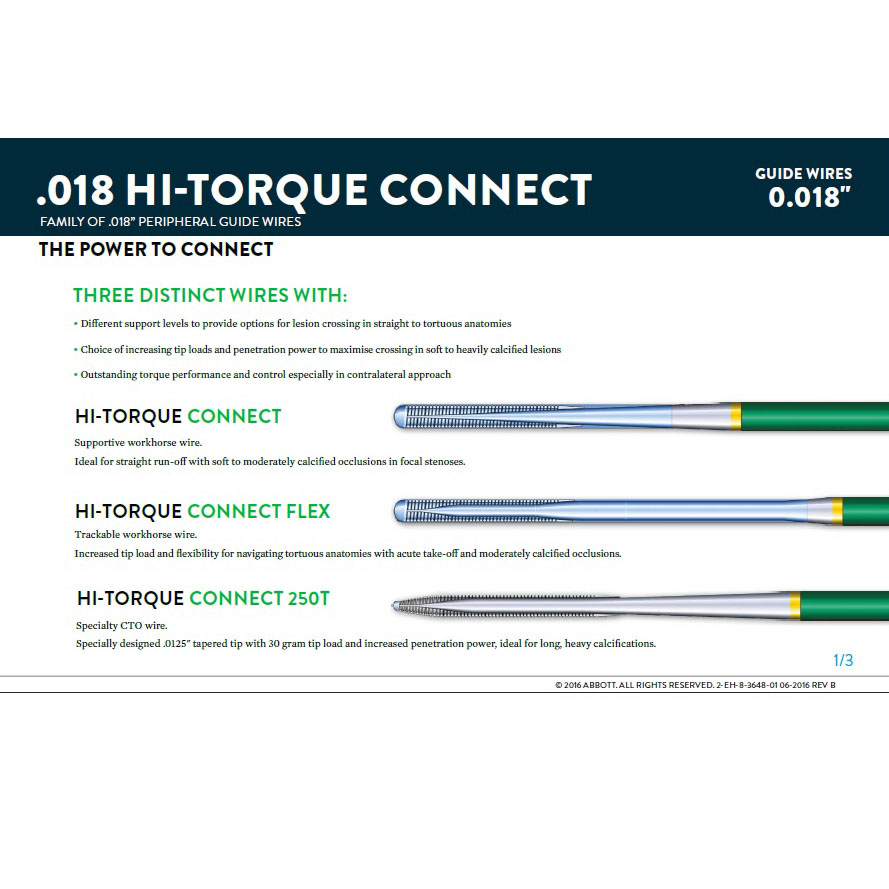
Hi-Torque Connect 0.018" Guide Wire Family / Abbott
A family of 0.018” wires designed for lower-limb anatomy with options for:


Our Cases of the Month
The case of the month is a new way for our users to watch, learn, and share with incathlab. They can watch a video that highlights an innovative case and uses excellent pedagogical techniques, lear...
Share
Join the Discussion
Suggestions
Complex Acute Anterior STEMI with "no Reflow phenomenon" management
Case of the month: October 2018
Share
Common femoral artery stenosis treated with directional atherectomy and DCB
Dr Schmidt, Dr van den Berg & Dr Bisdas
Share
Provisional Bifurcation techniques to support bailout scenarios
Insights from the Visible Heart�...
Case of the month: July 2024
Share
Occluded instent left SFA stenosis | Fractured stents treated - Eluvia stenting
Case of the month: June 2022
Share
Long Femoral Occlusion (35 cm) - Subintimal crossing and extra long stenting
Case of the month: July 2017
Share

Live case #5 from Swiss CTO Summit 2019 - Dr Avran & Dr Faurie
Case of the month: February 2020
Share
Simultaneous treatment of two coronary artery bifurcations in three vessels disease patient
Dedicated coronary bifurcation stents - Case of the month: May 2018
Share
{kind=link}
{kind=link}
venkatesa reddy D. very good result
Mangesh T. My few questions about about Long Calcified SFA Recanalisation-
1.What was the prime aim of this Interventions to treat Proximal SFA Occlusion with Directional Atherectomy or Short segment occluded SFA?
2.Is Pre-dilatation with Coronary balloons (1.5-3.5mm) always necessary before Debulking of Femoro-Popliteal lesion with Atherectomy device?
3.Exact role of Chocolate Cutting balloon could not be understud? Why so many wires & balloons are used instead of doing Straightforward Hawkone Atherectomy and then Drug coated balloon plasty with In.pact Admiral?
4.Is their any loss of Paclitexel drug while doing Balloon Plasty multiple times?
5. After 'Inline flow' Recanalisation Why not below the knee Popliteo-tibial revascularisation Not attempted in same seating?
6.Does ABI Improved after long SFA Recanalisation & return of triphasic waveform in tibial arteries?
I feel Distal Embolisation protection device has No role in this Atherectomy + DEB Case!
So many hardware material uses is Luxury for IR Consultant!!
Do you agree with my comments?
Mangesh T. Great case done. Amazing results!!
Alexandre P. Interesting, than you