×
It looks like you're using an obsolete version of internet explorer. Internet explorer is no longer supported by Microsoft since the end of 2015. We invite you to use a newer browser such as Firefox, Google Chrome or Microsoft Edge.
My Player placeholder

Become an Incathlab member and receive full access to its content!

You must be an Incathlab member to access videos without any restrictions. Register for free in one minute and access all services provided by Incathlab.You will also be able to log into Incathlab from your Facebook or twitter account by clicking on login on the top-right corner of Incathlab website.
Registration Login
Registration Login
Protocol
- Procedure time: 165 min
- Exposure time: 36 min
- Exposure: 349 mGray
-
Contrast volume: 2000 ml
Shooting date : 2018-06-29
Last update : 2021-06-09
Last update : 2021-06-09


Join the Discussion
Suggestions
Attempted recanalization of chronically thrombosed limb of Iliocaval reconstruction
Dr Thulasidasan & Dr Karunanithy
Share
Recanalisation and stenting of chronically-occluded right iliac veins in a patient with severe post-...
Dr Thulasidasan & Dr Karunanithy
Share
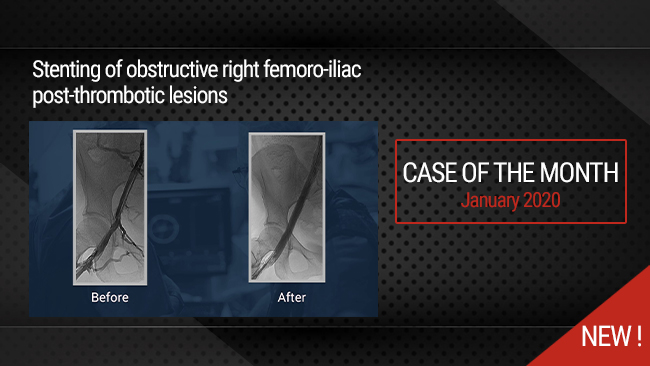
Stenting of obstructive right femoro-iliac post-thrombotic lesions
Case of the month: January 2020
Share
Up-and-over SAFARI to recanalize and stent a long-segment BTK occlusion in a patient with CLOI
Dr Thulasidasan & Dr Karunanithy
Share
Introducing Innovative Dual-Layer Technology for Fempop lesions
Case of the month : December 2024
Share
{kind=link}
K R. Why did we deploy stent in pop ata and tpt. There is no flow limiting dissection or >30% residual lesion in pop and tibial vessels after plasty. You could have left it there. Leaving even non flow limiting dissection is acceptable in tibials. The idea behing doing BTK is just to heal the foot lesion which could be achieved with plasty alone as you did
Deploying stent actually adds time, contrast and radiation exposure , cost on procedure. Does not any therapeutic benefit. And one more thing no need for DCB plasty for tibials.
mohamad ali A. its a good point i guess he wouldnt deploy it if there wasnt a plan of kissing for ata and tpt
Venkatesa R. very good