×
It looks like you're using an obsolete version of internet explorer. Internet explorer is no longer supported by Microsoft since the end of 2015. We invite you to use a newer browser such as Firefox, Google Chrome or Microsoft Edge.

Become an Incathlab member and receive full access to its content!

You must be an Incathlab member to access videos without any restrictions. Register for free in one minute and access all services provided by Incathlab.You will also be able to log into Incathlab from your Facebook or twitter account by clicking on login on the top-right corner of Incathlab website.
Registration Login
Registration Login
39896 views
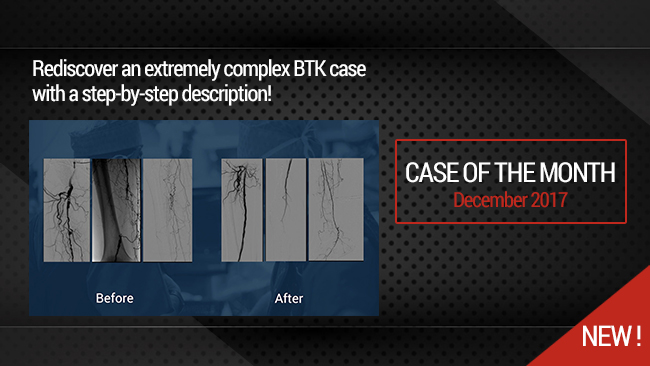
This 18 minutes didactic procedure concerns a 78 years old male with extremely severe peripheral artery disease: a Left limb amputation and a Right limb trophic ulcer. He presents Three right consecutive artery occlusions: Mid-SFA, Popliteal, proximal and distal posterior tibial.
This extremely complex case was treated using different technics according to the arterial segment: Sub intimal angioplasty and long stenting for SFA, Drug coated balloon for Popliteal, DES for proximal posterior tibial and coronary technics for plantar arteries.
Step-by-Step Procedure
- Right Antegrade femoral access
- Pre-procedure discussion of strategy for a multilevel artery occlusion
- Guide wire selection and escalation for crossing
- Support micro-catheter selection
- Pre-dilatation of more than 50cm with low profile long balloon
- Technics to re--enter in foot arteries
- DES for distal leg arteries
- DCB for popliteal artery
- Self-expandable drug eluting stent for dissection and residual stenosis of SFA
Learning points
- Selection and feasibility of antegrade femoral access
- Guide Wire and micro-catheter selection for multilevel crossing
- Balloon angioplasty with low profile long balloons
- Technics to re-enter in plantar artery
- Use of DCB (Drug Coated Balloon) for popliteal artery
- Use of balloon DES in tibial artery
- Self -expandable DES at the femoral level
Biobliography
-
Short-Term Results of Eluvia™ Paclitaxel-Eluting Stent in External Iliac and Femoropopliteal Lesions - Article
Elens M, Verhelst R, Possoz J, Mastrobuoni S, Lacroix V, Astarci P.
Surg Technol Int. 2017 Nov 9;31. pii: sti31/894. [Epub ahead of print]
-
Drug-coated balloon angioplasty for the management of recurring infrapopliteal disease in diabetic patients with critical limb ischemia - Article
Palena LM, Diaz-Sandoval LJ, Gòmez Jabalera E, Peypoch Perez O, Sultato E, Brigato C, Brocco E, Manzi M.
Cardiovasc Revasc Med. 2017 Jun 20. pii: S1553-8389(17)30196-3. doi: 10.1016/j.carrev.2017.06.006. [Epub ahead of print]
-
Innovations in the Endovascular Management of Critical Limb Ischemia: Retrograde Tibiopedal Access and Advanced Percutaneous Techniques - Article
Mustapha JA, Diaz-Sandoval LJ, Saab F.
Curr Cardiol Rep. 2017 Aug;19(8):68. doi: 10.1007/s11886-017-0879-1.
-
Innovations in the Endovascular Management of Critical Limb Ischemia: Retrograde Tibiopedal Access and Advanced Percutaneous Techniques - Article
Mustapha JA, Diaz-Sandoval LJ, Saab F.
Curr Cardiol Rep. 2017 Aug;19(8):68. doi: 10.1007/s11886-017-0879-1.
-
Angiosome-directed revascularization in patients with critical limb ischemia - Article
Jongsma H, Bekken JA, Akkersdijk GP, Hoeks SE, Verhagen HJ, Fioole B.
J Vasc Surg. 2017 Apr;65(4):1208-1219.e1. doi: 10.1016/j.jvs.2016.10.100.
Shooting date : 2016-12-05
Last update : 2018-01-31
Last update : 2018-01-31



Our Cases of the Month
The case of the month is a new way for our users to watch, learn, and share with incathlab. They can watch a video that highlights an innovative case and uses excellent pedagogical techniques, lear...
Share
Join the Discussion
Suggestions

Thursday, September 7th 2017 from 12pm to 01:30pm (GMT+2)
Honolulu : Thursday, September 7th 2017 from 01am to 02:30am (GMT+2)
San Francisco : Thursday, September 7th 2017 from 04am to 05:30am (GMT+2)
New York : Thursday, September 7th 2017 from 07am to 08:30am (GMT+2)
Buenos Aires : Thursday, September 7th 2017 from 08am to 09:30am (GMT+2)
Reykjavik : Thursday, September 7th 2017 from 11am to 12:30pm (GMT+2)
London / Dublin : Thursday, September 7th 2017 from 12pm to 01:30pm (GMT+2)
Paris / Berlin : Thursday, September 7th 2017 from 01pm to 02:30pm (GMT+2)
Istanbul : Thursday, September 7th 2017 from 02pm to 03:30pm (GMT+2)
Moscou / Dubaï : Thursday, September 7th 2017 from 03pm to 04:30pm (GMT+2)
Bangkok : Thursday, September 7th 2017 from 06pm to 07:30pm (GMT+2)
Shanghai : Thursday, September 7th 2017 from 07pm to 08:30pm (GMT+2)
Tokyo : Thursday, September 7th 2017 from 08pm to 09:30pm (GMT+2)
Sydney : Thursday, September 7th 2017 from 10pm to 11:30pm (GMT+2)
Wellington : Friday, September 8th 2017 from 12am to 01:30am (GMT+2)
San Francisco : Thursday, September 7th 2017 from 04am to 05:30am (GMT+2)
New York : Thursday, September 7th 2017 from 07am to 08:30am (GMT+2)
Buenos Aires : Thursday, September 7th 2017 from 08am to 09:30am (GMT+2)
Reykjavik : Thursday, September 7th 2017 from 11am to 12:30pm (GMT+2)
London / Dublin : Thursday, September 7th 2017 from 12pm to 01:30pm (GMT+2)
Paris / Berlin : Thursday, September 7th 2017 from 01pm to 02:30pm (GMT+2)
Istanbul : Thursday, September 7th 2017 from 02pm to 03:30pm (GMT+2)
Moscou / Dubaï : Thursday, September 7th 2017 from 03pm to 04:30pm (GMT+2)
Bangkok : Thursday, September 7th 2017 from 06pm to 07:30pm (GMT+2)
Shanghai : Thursday, September 7th 2017 from 07pm to 08:30pm (GMT+2)
Tokyo : Thursday, September 7th 2017 from 08pm to 09:30pm (GMT+2)
Sydney : Thursday, September 7th 2017 from 10pm to 11:30pm (GMT+2)
Wellington : Friday, September 8th 2017 from 12am to 01:30am (GMT+2)
The best choice in SFA procedures depending on multiple factors (Live Session)
Clinical - Anatomical - Cost efficiency
Share
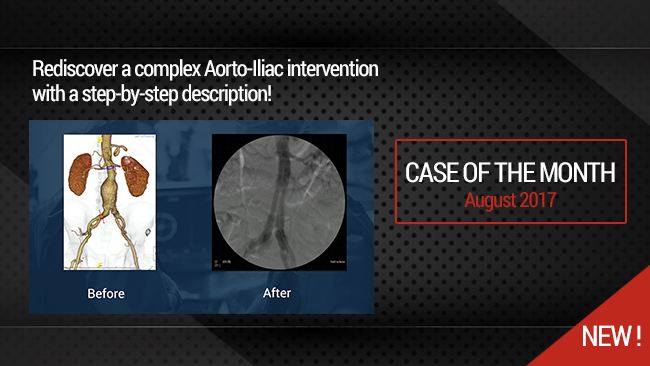
Percutaneous EndoVascular Aortic Repair (PEVAR) with low profile endovascular graft
Case of the month: August 2017
Share
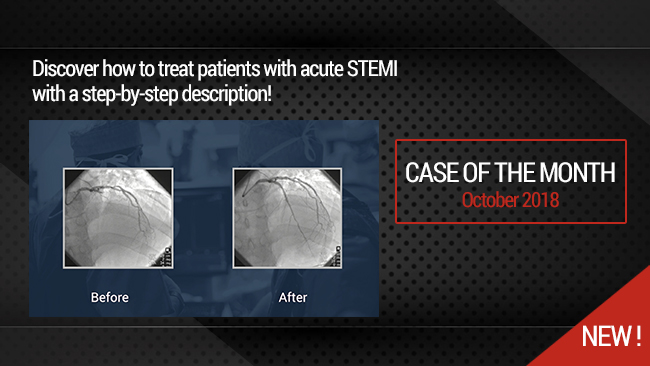
Complex Acute Anterior STEMI with "no Reflow phenomenon" management
Case of the month: October 2018
Share
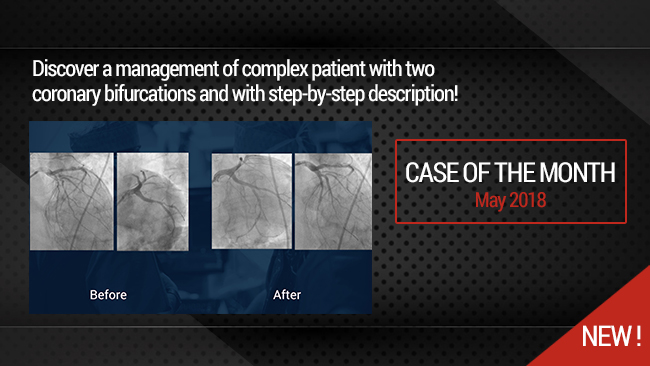
Simultaneous treatment of two coronary artery bifurcations in three vessels disease patient
Dedicated coronary bifurcation stents - Case of the month: May 2018
Share
Calcified distal Left Main and LAD stenoses - Rotablation treatment and IVUS evalutation
Case of the month: June 2017
Share
Progressive Right Internal Carotid Stenosis with Left Internal Carotid Artery Occlusion
Case of the month: November 2017
Share

{kind=link}
{kind=link}
{kind=link}
Alaaeldin H. what is the expected patency for this long segment ,multilevel occlusion.
Max A. Thank you for your comment. This patient requires a monthly follow up to maintain patency in order to assure ulcer healing . After 6 months the risk of restenosis and occlusion is high .
marcus P. Set good
Sandeep S. why did we have to break the end of Eluvia stent towards the end of deployment.
Georgi G. Leave a new comment to the discussion
Max A. It appears to be more convenient in long ELUVIA stent.
Collu B. Congratulations for very informative case