
Become an Incathlab member and receive full access to its content!

Registration Login
This month, we present the case of an 80 years old male patient, smoker, known to have HFrEF secondary to a cardiac amyloidosis TTR s/p CRT-D, severe aortic stenosis (ASA 0.6 cm2), hypertension, dyslipidemia and chronic kidney disease.
Coronary angiography pre-TAVR revealed: dominated RCA that is occluded as well as a moderate lesion of the obtuse marginal and severely calcified lesions of the proximal and mid LAD that is occluded distally.
Educational objectives
- How to manage a high-risk patient with multiple co-morbidities.
- Plan a step-by-step approach procedure for calcified lesion preparation and stenting.
- Choice of material: introducer size, guidewires, guide extension, choice of lesion modifying technique/tools.
- Role of intravascular imaging.
Step-by-step procedure:
1) Access site and hemodynamic stability:
- Right radial approach: 7 French EBU 3.5 to the left main.
- Under Dobutamine IV infusion.
- Anticoagulation using heparin.
2) Intravascular imaging:
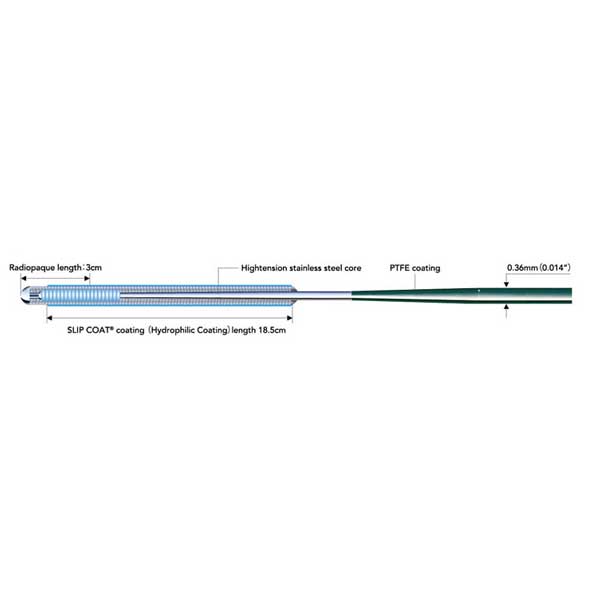
- Two 0.014” Sion Blue (Asahi) guidewires for extra support were introduced into the LAD.
- Intravascular imaging using optical frequency domain imaging (OFDI) (Terumo) at 40 mm/sec in order to minimize contrast injection showed superficially calcified LAD with several calcified nodules at the mid-LAD level and 360° calcium rings.
3) Calcium modifying device:
- Intravascular lithotripsy using a 3.5 x 12 mm Shockwave balloon was selected and the mid-LAD and proximal LAD lesions were predilated.
- Upon balloon inflations, a drop of blood pressure was noted, a small dose of Noradrenaline was set up.
- Further lesion preparation using a non-compliant balloon 3.5 mm inflated up to 20 atm was done at the level of the mid and proximal LAD lesions.
4) LAD stenting:
- A 3.5 x 21 mm Nagomi Ultimaster (Terumo) stent could not cross the proximal LAD lesion.
- A 6 French (due to out-of-stock 7 French) Boosting guide extension catheter (QX Medical) was introduced to the mid-LAD and facilitated stent delivery to the mid-LAD lesion that was inflated to 16 atm.
- Using the stent balloon, the guide extension catheter was advanced into the recently implanted stent.
- A 4.0 x 33 mm Nagomi Ultimaster (Terumo) was then implanted to cover the proximal LAD lesion and inflated to 16 atm.
5) Stent optimization:
- An OFDI run was performed at this time in order to assess the implanted stents and showed stent malapposition at different levels as well as a small dissection.
- Post-dilatation of the distal stent using a 4.0 mm non-compliant balloon inflated at 20 atm followed by a post-dilatation of the proximal stent using a 4.5 mm non-compliant balloon inflated at 20 atm were performed.
- The angiographic end-result was perfect.
6) Post-procedure patient care:
- Dobutamine tapering to stop over the next hour.

Bibliography
Last update : 2024-03-22




Live Case 4C 2023
6e Edition 4C 2023 JEUDI 21 SEPTEMBRE SESSION #1: L'OCT DANS LE STENTING FAILURE Modérateurs : Matthieu Godin & Nic...

Our Cases of the Month
The case of the month is a new way for our users to watch, learn, and share with incathlab. They can watch a video that highlights an innovative case and uses excellent pedagogical techniques, lear...
Join the Discussion
Suggestions
San Francisco : Tuesday, April 27th 2021 from 07am to 08am (GMT+2)
New York : Tuesday, April 27th 2021 from 10am to 11am (GMT+2)
Buenos Aires : Tuesday, April 27th 2021 from 11am to 12pm (GMT+2)
Reykjavik : Tuesday, April 27th 2021 from 02pm to 03pm (GMT+2)
London / Dublin : Tuesday, April 27th 2021 from 03pm to 04pm (GMT+2)
Paris / Berlin : Tuesday, April 27th 2021 from 04pm to 05pm (GMT+2)
Istanbul : Tuesday, April 27th 2021 from 05pm to 06pm (GMT+2)
Moscou / Dubaï : Tuesday, April 27th 2021 from 06pm to 07pm (GMT+2)
Bangkok : Tuesday, April 27th 2021 from 09pm to 10pm (GMT+2)
Shanghai : Tuesday, April 27th 2021 from 10pm to 11pm (GMT+2)
Tokyo : Tuesday, April 27th 2021 from 11pm to 12am (GMT+2)
Sydney : Wednesday, April 28th 2021 from 01am to 02am (GMT+2)
Wellington : Wednesday, April 28th 2021 from 03am to 04am (GMT+2)
{kind=link}
{kind=link}
v22e V. visiteur2@altilab.com