×
It looks like you're using an obsolete version of internet explorer. Internet explorer is no longer supported by Microsoft since the end of 2015. We invite you to use a newer browser such as Firefox, Google Chrome or Microsoft Edge.
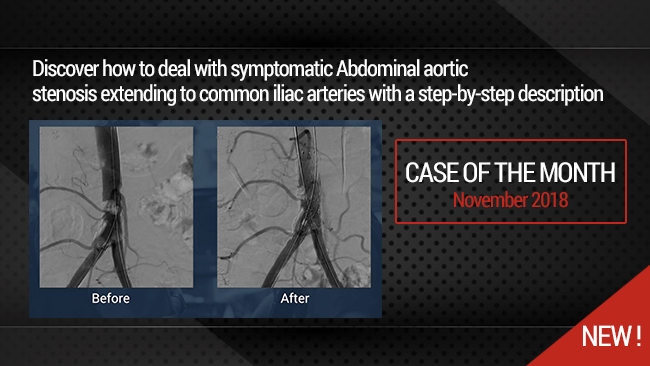
Complex Aorto-iliac lesion: How to deal with symptomatic Abdominal Aortic calcified stenosis extending to common iliac arteries
Case of the Month: November 2018
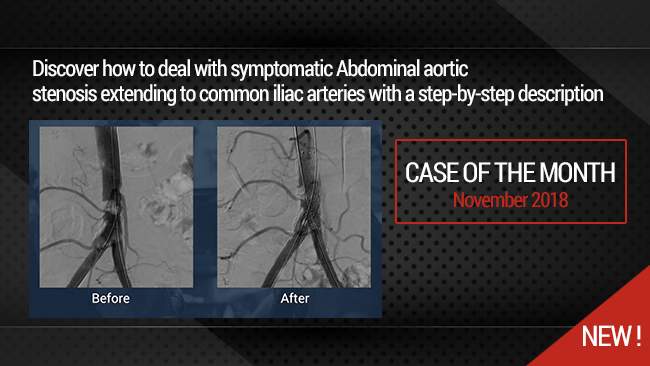
This didactic procedure concerns a young heavy smoker lady with bilateral lower limb severe claudication, presenting distal abdominal aortic calcified stenosis extending to bilateral common iliac arteries. After multimodality assessment of lesions, she has undergone percutaneous abdominal aortic & bilateral iliac angioplasty and stenting with good final result.
Educational objectives
- How to manage patients with intermittent claudication and Aorto-iliac stenosis.
- Multimodality assessment of aorto-iliac stenosis before the intervention.
- How to plan access, procedural steps, and selection of devices.
- How to preserve inferior mesenteric artery during distal abdominal aortic stenting.
Step-by-Step description
- Selection of femoral site: Left Femoral artery access with 7F 23cm introducer.
- Right Femoral artery access under Roadmap guidance (6F 23cm introducer).
- Crossing both iliac arteries & Aortic stenosis with 0.035" Advantage guidewire (Terumo).
- Aortic predilatation with a 10x40mm at 8ATM.
- Autoexpandable Stent implantation in the distal Aorta under Roadmap guidance: OPTIMED 12X40mm over the 7F Sheath.
- Recross the aortic stent with the right 0.035" guidewire.
- Simultaneous deployment of Two covered stents in both common iliac arteries BEGRAFT(Bentley): 7x37mm il the right side & 7x27mm in the left side.
- Kissing balloon with the stent balloons.
- Angiographic control in different views with good inferior mesenteric artery patency.
- Bilateral femoral arteries manual compression.
Biobliography
-
2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS) - Article
Authors: Victor Aboyans, Jean-Baptiste Ricco, Marie-Louise E L Bartelink
Publication: [DOI: 10.1016/j.ejvs.2017.07.018
-
Authors: Taeymans K, Goverde P, Lauwers K, Verbruggen P.Publication: 2016 Jun;57(3):343-9. Epub 2016 Mar 24
-
Strategies for managing aortoiliac occlusions: access, treatment and outcomes - Article
Authors: Daniel G Clair, and Jocelyn M Beach
Publication: doi: [10.1586/14779072.2015.1036741]
-
A systematic review of endovascular treatment of extensive aortoiliac occlusive disease - Article
Authors: Vincent Jongkind & al.
Publication: doi.org/10.1016/j.jvs.2010.04.080
-
- Article
Authors : Beate Maria Stoeckelhuber & al.
Publication: J Vasc Interv Radiol 2003; 14:1443–1447
-
Long-term Results of Primary Stent Placement to Treat Infrarenal Aortic Stenosis - Article
Authors: P.C.G.Simons & al.
Publication: doi.org/10.1016/j.ejvs.2006.05.010
Related videos
Complex Aorto-iliac lesion: How to deal with symptomatic Abdominal Aortic calcified stenosis extendi...
Case of the month: November 2018
Share
Related playlists

Our Cases of the Month
The case of the month is a new way for our users to watch, learn, and share with incathlab. They can watch a video that highlights an innovative case and uses excellent pedagogical techniques, lear...
Share
{kind=link}